Atrial structure
Feature summary
Left atrial diameters and areas
Long-axis LA chamber size from segmentation-derived diameters and planimetered mask areas.
Family: structuralUnit family: cm, cm²Source: Cine long-axis CMRPrimary output group: LA diameters and areasHypertrophic obstructive cardiomyopathy (I42.1)Atrial fibrillation and flutter (I48)Cerebral infarction (I63)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Left atrial volume
Biplane area-length LA volume curve summarized by maximum and minimum volume.
Heart failure (I50)Atrial fibrillation and flutter (I48)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Left atrial sphericity index
Shape index comparing maximum LA volume with a sphere defined by the largest LA diameter.
Family: structuralUnit family: unitlessSource: Cine long-axis CMRPrimary output group: LA sphericity indexAtrial fibrillation and flutter (I48)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Right atrial size
4-chamber RA diameters, areas, and single-plane area-length volume outputs.
Family: structuralUnit family: cm, cm², mLSource: Cine long-axis CMRPrimary output group: RA 4ch sizePulmonary heart disease (I27)Tricuspid valve disorders (I36)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.
Atrial structure phenotypes describe left and right atrial chamber size from cine long-axis CMR. This pilot page separates scientific evidence from CardiacNexus implementation provenance: scientific statements use inline citations, while exact column names and source-code behavior are recorded as implementation provenance rather than bibliography.
- Modality
- Cine long-axis CMR
- UKB source
- Data Field 20208
- Pipeline step
- Long-axis atrial segmentation and area-length measurement
- Outputs
- atrial_volume.csv, timeseries/atrium.npz, landmark/atrium_*.vtk, atrial QC plots
- Maturity
- Pilot source-audited phenotype page
Clinical question
Clinicians and paper readers inspect atrial size to understand chamber remodeling, loading history, and atrial disease substrate. LA size and function are described in the literature as markers of diastolic dysfunction, atrial fibrillation, and prognosis, but CardiacNexus structural measurements are not diagnostic rules or treatment thresholds [4] [7].
Use this page for LA/RA diameters, long-axis areas, LA biplane volume, RA 4-chamber volume, BSA-indexed structural outputs, and LA sphericity. Use Atrial function for emptying fractions, expansion index, pre-atrial-contraction volume, and peak emptying rates.
Disease badges in the feature summary are literature-context navigation aids. They are not CardiacNexus disease classifiers, diagnostic thresholds, or validated phenotype-to-ICD association results. Badge tooltips give only the short relation type; detailed interpretation remains in disease primers and the Disease interpretation section below.
Structural versus functional remodeling
Large atrial size is a structural remodeling marker. It does not determine whether reservoir, conduit, or booster-pump function is abnormal; those functions require atrial volume-time or strain-derived phenotypes [4].
Anatomical and physiological definition
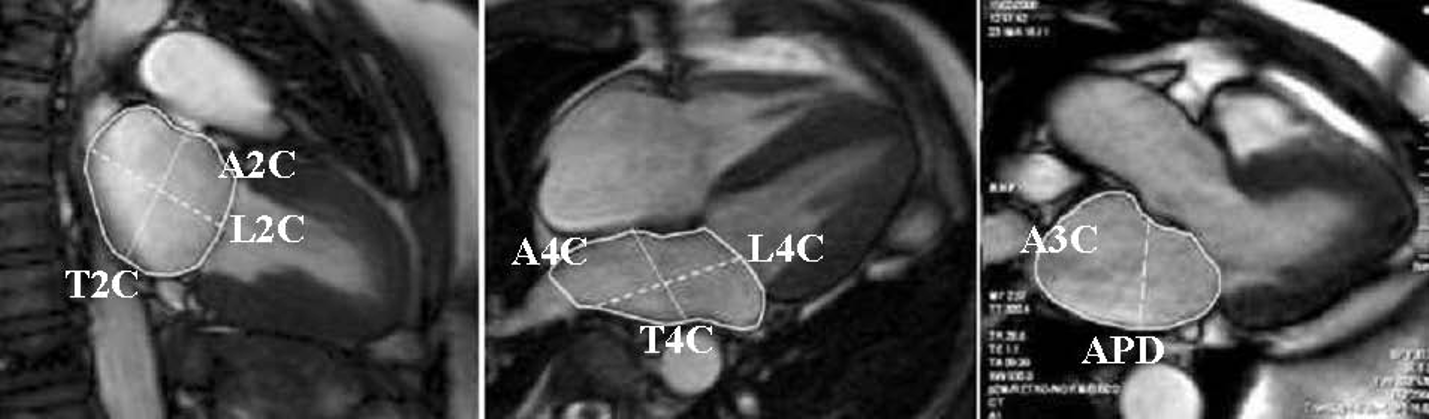
The LA CMR reference protocol measured areas in 2-chamber, 4-chamber, and 3-chamber/LVOT views, with longitudinal and transverse diameters in the 2-chamber and 4-chamber views at the end-systolic phase used for maximum atrial size [1]. CardiacNexus follows the 2-chamber and 4-chamber long-axis families: it reports LA longitudinal and transverse diameters in both views, and LA maximum/minimum areas in both views.
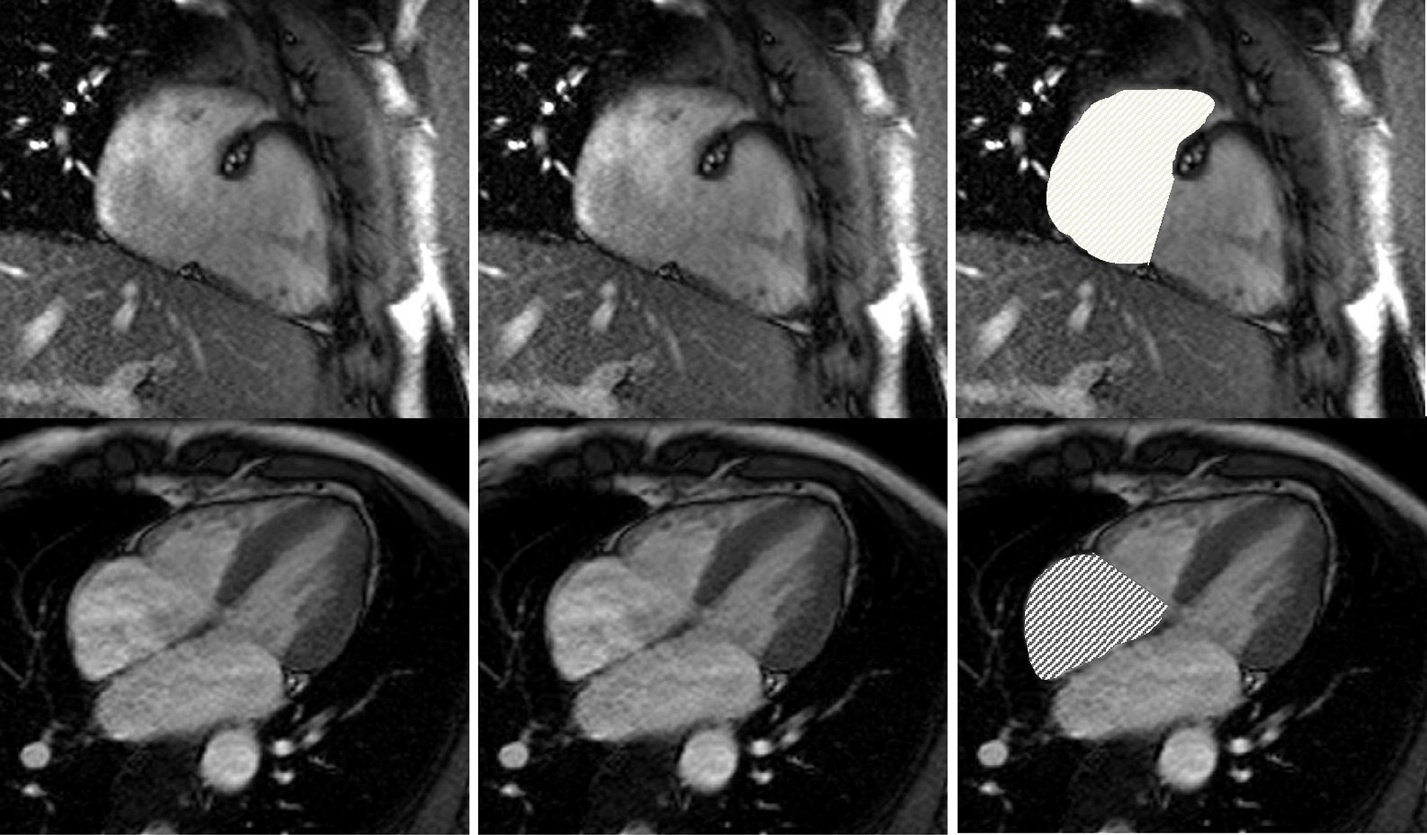
The RA reference protocol defines RA longitudinal diameter from the tricuspid-valve insertion midpoint toward the atrial roof and transverse diameter perpendicular to the longitudinal axis; it also emphasizes normalization by sex, BSA, and age where appropriate [2]. CardiacNexus currently derives RA structural measurements from the 4-chamber long-axis segmentation only.
LA volume has method-sensitive boundary conventions. Some CMR studies include the LA appendage and exclude pulmonary veins, while others exclude both the LA appendage and pulmonary veins for biplane or Simpson-style measurements [1] [3]. CardiacNexus does not independently encode a universal appendage or pulmonary-vein rule in this page; the public interpretation should be tied to the segmentation boundary used for each dataset.
Source acquisition and UKB field
The current structural extraction uses UK Biobank cine long-axis CMR, UK Biobank Data Field 20208. Full extraction expects sa.nii.gz, la_2ch.nii.gz, la_4ch.nii.gz, seg_la_2ch.nii.gz, and seg_la_4ch.nii.gz. The short-axis affine is used to orient the long-axis landmark routine, while 2-chamber and 4-chamber segmentations provide the atrial masks used for areas and diameters. These are implementation-provenance claims from eval_atrial_volume.py and utils/cardiac_utils.py::evaluate_atrial_area_length, not scientific bibliography claims.
The UK Biobank CMR reference-range paper used 1.5T bSSFP cine acquisitions, long-axis views, and manual analysis of all four chambers in a healthy Caucasian subset aged 45-74 years [6]. Those reference ranges are useful UKB context, but they should not be treated as CardiacNexus-specific normal limits unless the measurement convention and output definition match.
What exactly CardiacNexus measures
LA diameters and areas definition
For each frame, CardiacNexus takes the largest connected atrial label in the long-axis segmentation, computes mask area, finds a segmentation-derived longitudinal axis, and then measures a transverse diameter perpendicular to that axis at the atrial mid-level. The current implementation reports the maximum longitudinal and transverse diameters observed across frames. This implementation-specific route is registry-backed in docs/data/phenotype_dictionary.yml; it is not a universal CMR measurement convention.
For LA volume, CardiacNexus computes a biplane area-length estimate from the 2-chamber and 4-chamber areas and longitudinal lengths at each frame. LA: V_max (bip) [mL] and LA: V_min (bip) [mL] are the maximum and minimum of that framewise LA biplane curve.
RA 4ch size definition
For RA volume, CardiacNexus currently computes a single-plane 4-chamber area-length estimate from seg_la_4ch.nii.gz. It does not currently compute a biplane RA volume. The legacy indexed RA column names still include (bip) and are preserved as output-schema debt, not corrected in prose.
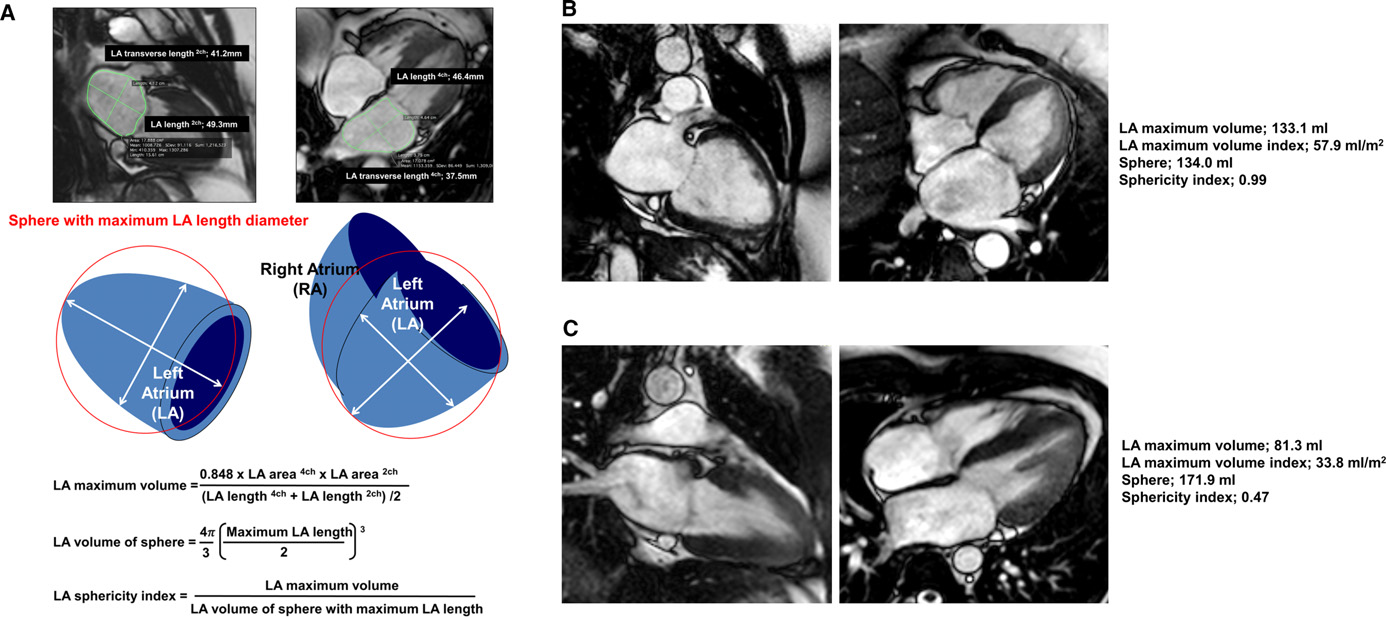
The LA sphericity index uses maximal LA volume divided by the volume of a sphere whose diameter is the largest LA longitudinal or transverse diameter among the 2-chamber and 4-chamber measurements. This follows the same geometric idea used in CMR sphericity-index studies, but remains sensitive to segmentation and landmark error [5].
Current output label debt
RA: V_max/BSA (bip) [mL/m^2], RA: V_min/BSA (bip) [mL/m^2], and RA: Volume (bip) [mL] are current compatibility labels. The implementation behind them is 4-chamber RA area-length estimation, not biplane RA measurement.
The BSA-indexed area columns keep the current labels A_max/BSA ... [mm^2/m^2] and A_min/BSA ... [mm^2/m^2]. The implementation divides area values documented in cm² by BSA, so the unit label should be treated as schema debt until a versioned output migration is approved.
Formula or computational route
LA biplane area-length volume
CardiacNexus computes LA biplane volume for each frame as:
Copyable formula
V_{LA,bip} = (8 / (3*pi)) * (A_{LA,4ch} * A_{LA,2ch}) / (0.5 * (L_{LA,4ch} + L_{LA,2ch}))| Variable | Meaning | Unit | Source view | Output mapping |
|---|---|---|---|---|
A_LA,2ch | LA area from the 2-chamber segmentation | cm² | seg_la_2ch.nii.gz | LA: A_max (2ch) [cm^2], LA: A_min (2ch) [cm^2] |
A_LA,4ch | LA area from the 4-chamber segmentation | cm² | seg_la_4ch.nii.gz | LA: A_max (4ch) [cm^2], LA: A_min (4ch) [cm^2] |
L_LA,2ch | LA longitudinal diameter in the 2-chamber view | cm | seg_la_2ch.nii.gz | LA: D_longitudinal (2ch) [cm] |
L_LA,4ch | LA longitudinal diameter in the 4-chamber view | cm | seg_la_4ch.nii.gz | LA: D_longitudinal (4ch) [cm] |
The implementation formula uses the mean of the 2-chamber and 4-chamber long-axis lengths. This is close to the published CMR sphericity study formula using a 0.848 coefficient and mean long-axis length [5]. It differs from biplane area-length conventions in other LA CMR work where the denominator can be the shorter long-axis length [3]. The page therefore labels CardiacNexus LA volume as an implementation-specific biplane area-length output, not a universal CMR reference value.
RA 4-chamber area-length volume
CardiacNexus computes RA volume for each frame from the 4-chamber view only:
Copyable formula
V_{RA,4ch} = (8 / (3*pi)) * A_{RA,4ch}^2 / L_{RA,4ch}| Variable | Meaning | Unit | Source view | Output mapping |
|---|---|---|---|---|
A_RA,4ch | RA area from the 4-chamber segmentation | cm² | seg_la_4ch.nii.gz | RA: A_max [cm^2], RA: A_min [cm^2] |
L_RA,4ch | RA longitudinal diameter from the 4-chamber segmentation | cm | seg_la_4ch.nii.gz | RA: D_longitudinal [cm] |
The current RA formula produces RA: V_max [mL], RA: V_min [mL], and the legacy NPZ key RA: Volume (bip) [mL]. It should be described as 4-chamber single-plane area-length estimation, even though some current indexed RA output labels still include (bip).
LA sphericity index
CardiacNexus computes LA sphericity index as:
Copyable formula
SI_{LA} = V_{LA,max} / ((4/3) * pi * (D_{LA,max} / 2)^3)| Variable | Meaning | Unit | Source view | Output mapping |
|---|---|---|---|---|
V_LA,max | Maximum framewise LA biplane volume | mL | seg_la_2ch.nii.gz, seg_la_4ch.nii.gz | LA: V_max (bip) [mL], numerator for LA: Sphericity_Index |
D_LA,max | Largest LA longitudinal or transverse diameter across 2-chamber and 4-chamber measurements | cm | seg_la_2ch.nii.gz, seg_la_4ch.nii.gz | LA diameter outputs feed the denominator |
The published sphericity method uses LA maximum volume divided by the volume of a sphere derived from the maximum LA length/diameter [5]. CardiacNexus follows that geometric route with its own segmentation-derived diameters and biplane volume curve. Because V_LA,max is reported in mL and D_LA,max is in cm, the denominator is also a cm³ volume; 1 cm³ equals 1 mL.
Measurement figures and provenance boundary
The figures below are source-paper panels extracted from the cited open-access PDFs for draft documentation development. They are displayed because they clarify measurement conventions, but their reuse permission and release acknowledgement wording still need final review before public release packaging.
Output columns and units
CardiacNexus writes atrial structural features into atrial_volume.csv.
The output list below is backed by docs/data/phenotype_dictionary.yml and checked against docs/data/output_column_inventory.yml plus eval_atrial_volume.py by npm run validate:atrial-registry.
| Display family | Exact output column | Unit | Status | Schema note |
|---|---|---|---|---|
| LA diameter | LA: D_longitudinal (2ch) [cm] | cm | current | none |
| LA diameter | LA: D_longitudinal (4ch) [cm] | cm | current | none |
| LA diameter | LA: D_transverse (2ch) [cm] | cm | current | none |
| LA diameter | LA: D_transverse (4ch) [cm] | cm | current | none |
| LA BSA-indexed diameter | LA: D_longitudinal/BSA (2ch) [cm/m^2] | cm/m² | current | none |
| LA BSA-indexed diameter | LA: D_longitudinal/BSA (4ch) [cm/m^2] | cm/m² | current | none |
| LA BSA-indexed diameter | LA: D_transverse/BSA (2ch) [cm/m^2] | cm/m² | current | none |
| LA BSA-indexed diameter | LA: D_transverse/BSA (4ch) [cm/m^2] | cm/m² | current | none |
| LA area | LA: A_max (2ch) [cm^2] | cm² | current | none |
| LA area | LA: A_min (2ch) [cm^2] | cm² | current | none |
| LA area | LA: A_max (4ch) [cm^2] | cm² | current | none |
| LA area | LA: A_min (4ch) [cm^2] | cm² | current | none |
| LA BSA-indexed area | LA: A_max/BSA (2ch) [mm^2/m^2] | mm²/m² | current compatibility label | unit-label debt: implementation divides cm² by BSA |
| LA BSA-indexed area | LA: A_min/BSA (2ch) [mm^2/m^2] | mm²/m² | current compatibility label | unit-label debt: implementation divides cm² by BSA |
| LA BSA-indexed area | LA: A_max/BSA (4ch) [mm^2/m^2] | mm²/m² | current compatibility label | unit-label debt: implementation divides cm² by BSA |
| LA BSA-indexed area | LA: A_min/BSA (4ch) [mm^2/m^2] | mm²/m² | current compatibility label | unit-label debt: implementation divides cm² by BSA |
| LA volume | LA: V_max (bip) [mL] | mL | current | none |
| LA volume | LA: V_min (bip) [mL] | mL | current | none |
| LA BSA-indexed volume | LA: V_max/BSA (bip) [mL/m^2] | mL/m² | current | none |
| LA BSA-indexed volume | LA: V_min/BSA (bip) [mL/m^2] | mL/m² | current | none |
| LA geometry | LA: Sphericity_Index | unitless | current | none |
| RA diameter | RA: D_longitudinal [cm] | cm | current | none |
| RA diameter | RA: D_transverse [cm] | cm | current | none |
| RA BSA-indexed diameter | RA: D_longitudinal/BSA [cm/m^2] | cm/m² | current | none |
| RA BSA-indexed diameter | RA: D_transverse/BSA [cm/m^2] | cm/m² | current | none |
| RA area | RA: A_max [cm^2] | cm² | current | none |
| RA area | RA: A_min [cm^2] | cm² | current | none |
| RA BSA-indexed area | RA: A_max/BSA [mm^2/m^2] | mm²/m² | current compatibility label | unit-label debt: implementation divides cm² by BSA |
| RA BSA-indexed area | RA: A_min/BSA [mm^2/m^2] | mm²/m² | current compatibility label | unit-label debt: implementation divides cm² by BSA |
| RA volume | RA: V_max [mL] | mL | current 4ch output | none |
| RA volume | RA: V_min [mL] | mL | current 4ch output | none |
| RA BSA-indexed volume | RA: V_max/BSA (bip) [mL/m^2] | mL/m² | current compatibility label | (bip) label debt: implementation is 4ch-only |
| RA BSA-indexed volume | RA: V_min/BSA (bip) [mL/m^2] | mL/m² | current compatibility label | (bip) label debt: implementation is 4ch-only |
The same extraction script also emits atrial functional columns such as LA: EF_total [%], RA: EF_total [%], LA: EI [%], RA: EI [%], peak emptying rates, and ECG-dependent pre-atrial-contraction features. Those are documented on Atrial function.
timeseries/atrium.npz stores LA: Volume (bip) [mL], RA: Volume (bip) [mL], LA: T_max, and LA: T_min. LA: T_pre_a is written only when ECG-based pre-atrial-contraction timing is available and passes the current checks. The RA NPZ key keeps (bip) for compatibility, but the stored curve comes from the 4-chamber RA route above.
Schema debt migration note: the RA (bip) volume labels and the BSA-indexed area unit labels are current compatibility debt. Future cleanup must use a versioned output migration with downstream release notes, registry updates, documentation updates, and compatibility handling; these labels must not be silently renamed in existing CSV or NPZ outputs.
Required upstream inputs
Full structural extraction currently requires:
sa.nii.gzfor long-axis orientation context.la_2ch.nii.gzandseg_la_2ch.nii.gzfor LA 2-chamber area, length, transverse diameter, and biplane LA volume.la_4ch.nii.gzandseg_la_4ch.nii.gzfor LA 4-chamber measurements and RA 4-chamber measurements.- Body surface area from the configured external table for indexed columns.
Missing 2-chamber or 4-chamber segmentation prevents full structural extraction. BSA-indexed outputs require a valid BSA value. This is a current input-contract boundary, not a scientific reference-range rule.
The exact missing-BSA row behavior and conditional NPZ-writing behavior are developer provenance and are handled through the implementation table and registry checks rather than as clinical interpretation rules.
Reference ranges with cohort and method context
| Feature | Source cohort | Reference value | Method context | Verification status | Citation |
|---|---|---|---|---|---|
| LA longitudinal diameter, 4ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 5.7 cm, 95% CI 4.3-7.0 cm | Table 2 all-ages row maps conceptually to LA: D_longitudinal (4ch) [cm]; source uses manual end-systolic measurement, while CardiacNexus uses segmentation-derived maximum framewise diameter | Verified source | Maceira et al. 2010 [1] |
| LA longitudinal diameter, 2ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 4.9 cm, 95% CI 3.4-6.3 cm | Table 2 all-ages row maps conceptually to LA: D_longitudinal (2ch) [cm]; source uses manual end-systolic measurement | Verified source | Maceira et al. 2010 [1] |
| LA transverse diameter, 4ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 4.1 cm, 95% CI 3.0-5.1 cm | Table 2 all-ages row maps conceptually to LA: D_transverse (4ch) [cm]; source uses manual end-systolic measurement | Verified source | Maceira et al. 2010 [1] |
| LA transverse diameter, 2ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 4.6 cm, 95% CI 3.6-5.6 cm | Table 2 all-ages row maps conceptually to LA: D_transverse (2ch) [cm]; source uses manual end-systolic measurement and reports age effects | Verified source | Maceira et al. 2010 [1] |
| LA area, 4ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 21 cm², 95% CI 14-28 cm² | Table 2 all-ages row maps conceptually to LA: A_max (4ch) [cm^2]; source uses manual end-systolic planimetry | Verified source | Maceira et al. 2010 [1] |
| LA area, 2ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 20 cm², 95% CI 11-29 cm² | Table 2 all-ages row maps conceptually to LA: A_max (2ch) [cm^2]; source uses manual end-systolic planimetry | Verified source | Maceira et al. 2010 [1] |
| Other LA volumes, BSA-indexed rows, sex-specific strata, and age-specific strata | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | queued in reference_range_sources.yml | Source reports sex/BSA/age effects and 2ch/4ch/3ch views; unlisted exact rows remain queued for row-level display rather than omitted from the source audit | Needs verification | Maceira et al. 2010 [1] |
| RA longitudinal diameter, 4ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 5.5 cm, 95% CI 4.3-6.6 cm | Table 2 all-ages row maps conceptually to RA: D_longitudinal [cm]; source reports male/female strata and BSA-indexed rows, while CardiacNexus uses segmentation-derived maximum framewise 4ch diameter | Verified source | Maceira et al. 2013 [2] |
| RA transverse diameter, 4ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 4.7 cm, 95% CI 3.7-5.8 cm | Table 2 all-ages row maps conceptually to RA: D_transverse [cm]; source uses manual maximum-size 4ch measurement | Verified source | Maceira et al. 2013 [2] |
| RA area, 4ch | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 22 cm², 95% CI 15-30 cm² | Table 2 all-ages row maps conceptually to RA: A_max [cm^2]; source includes RA appendage and excludes cava veins | Verified source | Maceira et al. 2013 [2] |
| RA volume, 4ch/source-paper context | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | mean 100 mL, 95% CI 61-139 mL | Table 2 all-ages source-paper volume row is verified, but method matching is limited because CardiacNexus currently computes 4ch single-plane area-length RA volume | Verified source; method-dependent | Maceira et al. 2013 [2] |
| Other RA BSA-indexed rows, sex-specific strata, and age-specific strata | 120 healthy adults, 60 men/60 women, age deciles 20-80, 1.5T SSFP CMR | queued in reference_range_sources.yml | Source includes RA appendage/cava convention and 2ch rows; unlisted rows need method mapping before public numeric display | Needs verification | Maceira et al. 2013 [2] |
| LA biplane volume and phasic volume context | 31 post-stroke patients at 3T, biplane area-length versus Simpson comparison | not a normal range for CardiacNexus | Useful for formula/method limitation; not a healthy UKB reference range | Literature context | Wandelt et al. 2017 [3] |
| LA biplane maximum volume UKB context | 795 healthy Caucasian UKB participants in atrial analysis, 363 men/432 women, age 45-74, 1.5T bSSFP CMR | all 66 ± 19 mL; men 71 ± 19 mL; women 62 ± 17 mL | Table 13; manual HLA 4ch and VLA 2ch contours, biplane area-length volume. Age-specific Tables 8/9 and BSA-indexed rows remain context for stratified use, not CardiacNexus-specific limits | Verified source; UKB context | Petersen et al. 2017 [6] |
| LA biplane maximum volume index UKB context | 795 healthy Caucasian UKB participants in atrial analysis, 363 men/432 women, age 45-74, 1.5T bSSFP CMR | all 37 ± 10 mL/m²; men 36 ± 9 mL/m²; women 37 ± 10 mL/m² | Table 13; BSA-indexed manual biplane LA maximum volume, useful as UKB context for LA: V_max/BSA (bip) [mL/m^2] | Verified source; UKB context | Petersen et al. 2017 [6] |
| RA maximum volume, 4ch UKB context | 795 healthy Caucasian UKB participants in atrial analysis, 363 men/432 women, age 45-74, 1.5T bSSFP CMR | all 80 ± 25 mL; men 93 ± 27 mL; women 69 ± 17 mL | Table 13; manual 4ch RA maximum volume, useful UKB context for RA: V_max [mL]; not a CardiacNexus-specific limit | Verified source; UKB context | Petersen et al. 2017 [6] |
| RA maximum volume index, 4ch UKB context | 795 healthy Caucasian UKB participants in atrial analysis, 363 men/432 women, age 45-74, 1.5T bSSFP CMR | all 44 ± 12 mL/m²; men 48 ± 14 mL/m²; women 41 ± 10 mL/m² | Table 13; BSA-indexed manual 4ch RA maximum volume, useful UKB context for the current indexed RA volume output despite (bip) label debt | Verified source; UKB context | Petersen et al. 2017 [6] |
| LA sphericity index, matched controls | 20 age- and sex-matched controls in Nakamori et al. | mean 0.74 ± 0.09; no controls >0.87 | Control context for the published sphericity study; this is not a CardiacNexus normal range or diagnostic threshold | Literature context; verified source | Nakamori et al. 2018 [5] |
| LA sphericity index, PVI recurrence cohort | 227 AF patients undergoing first pulmonary vein isolation | baseline all 0.82 ± 0.11; no late recurrence 0.80 ± 0.11; late recurrence 0.86 ± 0.09; ROC cutoff 0.84 for 1-year recurrence in that cohort | Outcome-context row only; do not convert these cohort-specific recurrence values into a CardiacNexus disease classifier | Literature context; verified source | Nakamori et al. 2018 [5] |
Disease interpretation
Badge-level disease links are intentionally narrow: they describe relation types supported by source literature, not CardiacNexus disease calls or phenotype-to-ICD association results.
LA size, LA volume, and LA shape are remodeling markers. They can support a clinical narrative about diastolic loading, atrial fibrillation substrate, HCM-related remodeling, or thromboembolic/cerebrovascular context, but none of these measurements is a standalone diagnosis or treatment threshold [4] [7] [9].
LA sphericity is included as geometric remodeling context. It has been studied in AF cohorts and pulmonary-vein-isolation recurrence research, but its interpretation depends on source cohort, rhythm status, acquisition, and measurement method [5].
RA size is primarily a right-heart loading and remodeling marker on this page. Interpret it with RV size/function, pulmonary-pressure context, tricuspid-valve disease, rhythm information, BSA, and image quality rather than as an isolated disease label [2] [8] [9].
The Cerebral infarction (I63) badge is disabled until a stroke/cerebrovascular primer exists. It is retained only as AF-related thromboembolic context and must not link to ischemic heart disease or myocardial infarction.
Evidence mapping for disease-navigation badges
| Feature family | Badge | Relation type | Evidence status | Sources |
|---|---|---|---|---|
| LA diameters and areas | Hypertrophic obstructive cardiomyopathy (I42.1) | HCM diastolic/loading context | Literature context | [9] [4] |
| LA diameters and areas | Atrial fibrillation and flutter (I48) | AF / atrial remodeling context | Literature context | [4] [7] [9] |
| LA diameters and areas | Cerebral infarction (I63) | Cerebrovascular thromboembolic context | Literature context | [9] |
| LA volume | Heart failure (I50) | HF / diastolic loading context | Literature context | [4] [9] |
| LA volume | Atrial fibrillation and flutter (I48) | AF / atrial remodeling context | Literature context | [7] [9] |
| LA sphericity index | Atrial fibrillation and flutter (I48) | AF geometric remodeling context | Literature context | [5] |
| RA size | Pulmonary heart disease (I27) | Pulmonary hypertension / right-heart loading context | Literature context | [9] |
| RA size | Tricuspid valve disorders (I36) | Tricuspid valve / right-heart volume loading context | Literature context | [9] |
QC caveats and maturity boundary
Atrial measurements are sensitive to long-axis plane coverage, off-axis acquisition, atrial truncation, annular landmark placement, segmentation leakage, and boundary handling near pulmonary veins and atrial appendages. The scientific literature does not use one universally identical LA/RA boundary convention, and the CardiacNexus implementation follows the segmentation masks it receives [1] [3] [5].
The biplane area-length method is fast and compatible with routine 2-chamber and 4-chamber cine views, but it relies on geometric assumptions. Wandelt et al. found method-dependent differences between biplane area-length and Simpson-style volumetric LA assessment, so reference values from one method should not be mixed with another without explicit method context [3].
Implementation provenance
Implementation provenance supports current-output and schema claims only; it is not part of the scientific bibliography.
| Provenance item | Role | Current decision |
|---|---|---|
src/feature_extraction/Long_Axis_20208/eval_atrial_volume.py | Computes LA/RA areas, diameters, volume curves, BSA-indexed columns, functional columns, NPZ keys, and QC plots | Verified implementation source for this page |
utils/cardiac_utils.py::evaluate_atrial_area_length | Computes segmentation-derived area, longitudinal diameter, transverse diameter, and landmarks | Verified implementation source for landmark-dependent measurement route |
utils/quality_control_utils.py::atrium_pass_quality_control | Fails segmentation when atrial labels nearly vanish in any frame | Verified implementation source for a minimal segmentation QC caveat |
utils/biobank_utils.py::query_BSA | Reads configured BSA table for indexed columns | Verified implementation source for BSA dependency |
eval_atrial_volume.py missing-BSA branch | Current script skips the subject-level CSV row after basic time-series outputs have already been written if BSA lookup fails | Developer-facing behavior only; not a clinical interpretation rule |
docs/data/phenotype_dictionary.yml | Records Atrial structure canonical IDs, exact output columns, units, formula IDs, schema debt, clinician definitions, developer notes, and NPZ keys | Atrial-first output registry |
website/scripts/validate-atrial-registry.cjs | Checks the Atrial page, phenotype dictionary, output inventory, NPZ keys, and eval_atrial_volume.py agree | Registry consistency audit |
docs/data/output_column_inventory.yml | Records exact atrial_volume.csv columns, timeseries/atrium.npz keys, and schema debt | Output contract source |
docs/data/figure_provenance.yml | Records actual asset paths, source paper, figure/panel locator, extraction method, permission status, caption boundary, and review status for the displayed LA/RA/sphericity draft source figures | Figure provenance source |
| Formula anchors | Stable developer anchors for LA biplane volume, RA 4-chamber volume, and LA sphericity index formula blocks | Kept out of the main reading flow; use the section anchors near each formula for developer cross-reference |
docs/audits/source_claim_matrix.md and docs/audits/verification_queue.md | Track claim-level evidence, unsupported claims, and review status | Developer audit trail |
Source audit
This pilot page uses the refined source-audit workflow:
- Scientific references below contain only papers, review literature, and formal textbook references.
- Code paths and schema files are presented in Implementation provenance instead of References.
- Formula claims are rendered as KaTeX math blocks with variable, Unit, Source view, and Output mapping tables. Copy/search fallback text is kept in collapsed
Copyable formulacontrols and math accessibility labels, rather than repeated in the main reading flow. - Three source-paper figures are displayed from the page-local public image directory with draft permission-pending provenance: Maceira 2010 Figure 2 for LA measurement context, Maceira 2013 Figure 2 for RA measurement context, and Nakamori 2018 Figure 1 for LA sphericity context. The old atrial PNG paths and draft schematic SVG prototypes are not used on this page.
- The reference table now includes verified all-subject Maceira 2010 LA diameter/area rows, verified Maceira 2013 RA 4ch diameter/area/source-volume rows, Petersen 2017 UKB atrial volume context rows, and Nakamori 2018 LA sphericity context rows. Unlisted indexed, sex-specific, age-specific, and method-mismatched rows remain
Needs verification. - Atrial structure output columns are backed by
docs/data/phenotype_dictionary.ymland the registry consistency check. - Claims that still need source-level adjudication are tracked in
docs/audits/verification_queue.md. - Braunwald textbook background context for HFpEF, HCM, AF, stroke prevention, pulmonary hypertension, and valvular/tricuspid disease is summarized in the public source note below. The QA extraction details remain in
docs/audits/braunwald_atrial_structure_source_audit_2026-05-20.md.
Textbook context used on this page
Braunwald's Heart Disease, 12th ed. is used only as clinical background context here. It is not a CardiacNexus validation source, not a reference-range source, and not a diagnostic-rule source.
| Context | Braunwald chapter | Printed pages | How it is used |
|---|---|---|---|
| HFpEF / diastolic dysfunction | Heart Failure with Normal Ejection Fraction | 586-600 | LA enlargement and chronic loading / diastolic dysfunction context. |
| Hypertrophic cardiomyopathy | Hypertrophic Cardiomyopathy | 1582-1594 | LA remodeling, diastolic dysfunction, and AF context in HCM. |
| Atrial fibrillation | Atrial Fibrillation: Clinical Features, Mechanisms, and Management | 825-844 | AF substrate, LA remodeling, thromboembolic prevention, and left atrial appendage context. |
| Stroke prevention | Prevention and Management of Stroke | 1359-1367 | Cerebrovascular and thromboembolic context for atrial disease navigation. |
| Pulmonary hypertension | Pulmonary Hypertension | 1696-1718 | Right-heart loading context for RA enlargement interpretation. |
| Valvular / tricuspid disease | Valvular Heart Disease | 1468-1539 | Tricuspid and valvular volume-loading context for RA remodeling. |
Related pages
References
- Maceira AM, Cosin-Sales J, Roughton M, Prasad SK, Pennell DJ. Reference left atrial dimensions and volumes by steady state free precession cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance. 2010;12:65. doi:10.1186/1532-429X-12-65. PMID:21070636; PMCID:PMC2994941.
- Maceira AM, Cosin-Sales J, Roughton M, Prasad SK, Pennell DJ. Reference right atrial dimensions and volume estimation by steady state free precession cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance. 2013;15(1):29. doi:10.1186/1532-429X-15-29. PMID:23566426; PMCID:PMC3627628.
- Wandelt LK, Kowallick JT, Schuster A, Wachter R, Stumpfig T, Unterberg-Buchwald C, et al. Quantification of left atrial volume and phasic function using cardiovascular magnetic resonance imaging: comparison of biplane area-length method and Simpson's method. The International Journal of Cardiovascular Imaging. 2017;33(11):1761-1769. doi:10.1007/s10554-017-1160-9. PMID:28523471.
- Hoit BD. Left atrial size and function. Journal of the American College of Cardiology. 2014;63(6):493-505. doi:10.1016/j.jacc.2013.10.055. PMID:24291276.
- Nakamori S, Ngo LH, Tugal D, Manning WJ, Nezafat R. Incremental value of left atrial geometric remodeling in predicting late atrial fibrillation recurrence after pulmonary vein isolation: a cardiovascular magnetic resonance study. Journal of the American Heart Association. 2018;7(19):e009793. doi:10.1161/JAHA.118.009793. PMID:30371333; PMCID:PMC6404907.
- Petersen SE, Aung N, Sanghvi MM, Zemrak F, Fung K, Paiva JM, et al. Reference ranges for cardiac structure and function using cardiovascular magnetic resonance in Caucasians from the UK Biobank population cohort. Journal of Cardiovascular Magnetic Resonance. 2017;19(1):18. doi:10.1186/s12968-017-0327-9. PMID:28178995; PMCID:PMC5304550.
- Peters DC, Lamy J, Sinusas AJ, Baldassarre LA. Left atrial evaluation by cardiovascular magnetic resonance: sensitive and unique biomarkers. European Heart Journal - Cardiovascular Imaging. 2022;23(1):14-30. doi:10.1093/ehjci/jeab221. PMID:34718484; PMCID:PMC8685602.
- Lang RM, Cameli M, Sade LE, Faletra FF, Fortuni F, Rossi A, Soulat-Dufour L. Imaging assessment of the right atrium: anatomy and function. European Heart Journal - Cardiovascular Imaging. 2022;23(7):867-884. doi:10.1093/ehjci/jeac011. PMID:35079782.
- Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, editors. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia: Elsevier; 2022. Used here as background textbook context for HFpEF/diastolic dysfunction, hypertrophic cardiomyopathy, atrial fibrillation, stroke prevention, pulmonary hypertension, and valvular/tricuspid disease; not a CardiacNexus validation source. Public chapter and printed page spans are listed in the Textbook context source note above.