Cross-chamber phenotypes
Feature summary
Atrioventricular plane displacement
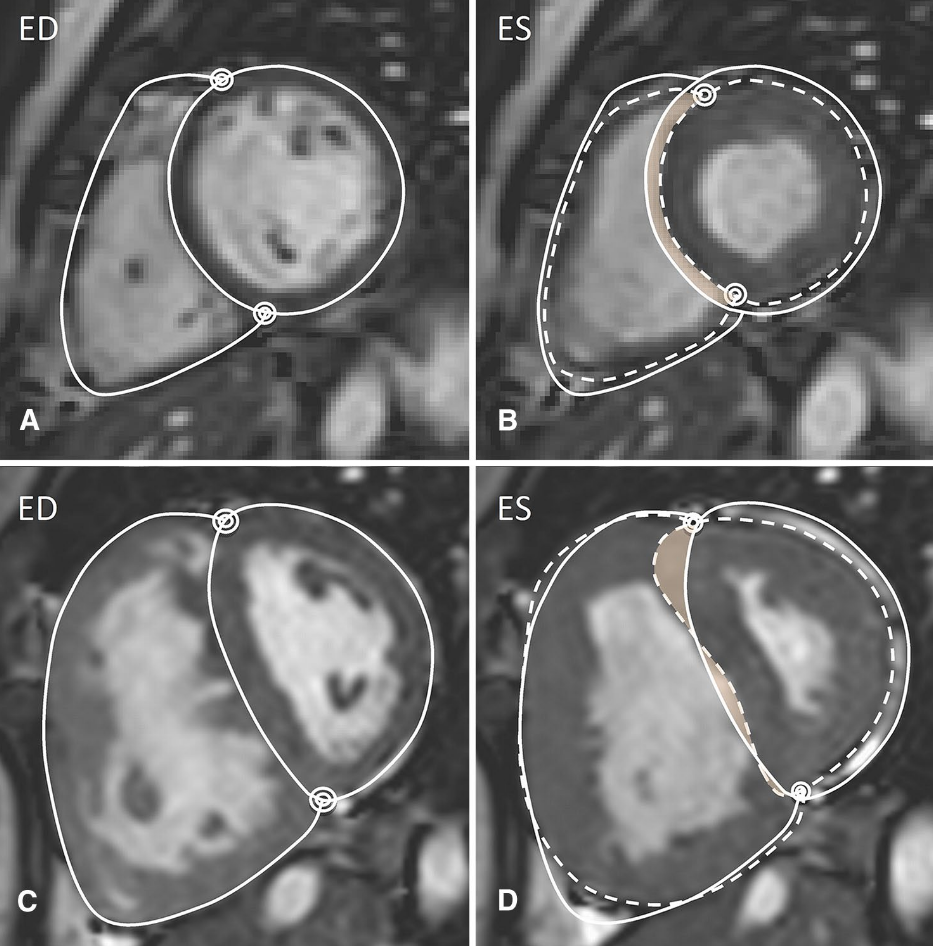
Simplified 4-chamber AV plane descent between ED and ES from the current combined-feature route.
Family: functionalUnit family: cmSource: Cine long-axis imagingPrimary output group: ventricular_atrial_feature.csvPrimary pulmonary hypertension (I27.0)Dilated cardiomyopathy (I42.0)Heart failure (I50)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Isovolumetric pulmonary vein transit
Difference between LV stroke volume and LA total stroke volume, plus ratio to LA total stroke volume.
Family: functionalUnit family: mL; ratioSource: Cine short-axis and long-axis imagingPrimary output group: ventricular_atrial_feature.csvDiastolic heart failure (I50.3)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Atrial contribution to LV filling
LV filling increment after the LA pre-atrial-contraction time point, normalized to LVSV or LVEDV.
Family: functionalUnit family: %Source: Cine short-axis and long-axis timingPrimary output group: ventricular_atrial_feature.csvAcute myocardial infarction (I21)Diastolic heart failure (I50.3)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Regional contribution to stroke volume boundary
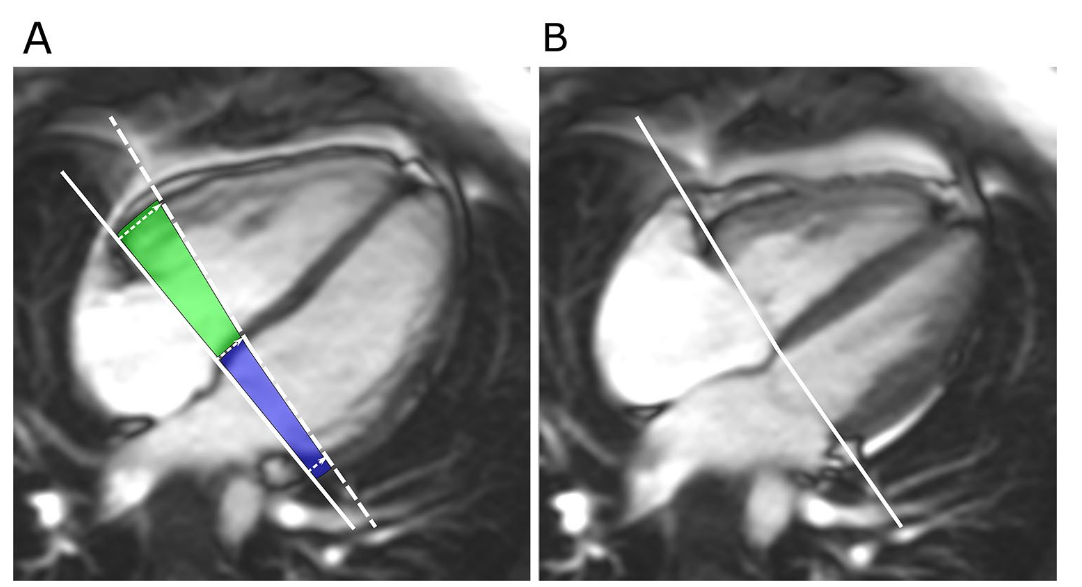
Regional longitudinal, septal, and lateral stroke-volume contribution is literature context only in this page.
Family: functionalUnit family: %, not current outputSource: Literature context onlyPrimary output group: not current outputPrimary pulmonary hypertension (I27.0)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.
Cross-chamber phenotypes combine ventricular and atrial measurements to describe chamber coupling, longitudinal pump function, and diastolic filling relationships. This page is source-audited for the current non-valvular ventricular_atrial_feature.csv rows. The same aggregate also contains mitral and tricuspid annular diameter rows, but those are documented on Valvular and flow phenotypes.
- Modality
- Cine short-axis CMR; cine long-axis CMR; ECG timing when available
- UKB source
- Data Fields 20208 and 20209, with ECG timing support
- Pipeline step
- Combined ventricular-atrial feature extraction
- Outputs
- ventricular_atrial_feature.csv, visualization/combined/AV_plane.png
- Maturity
- Source-audited phenotype page
Clinical question
Cross-chamber rows ask how atrial emptying, ventricular stroke volume, and atrioventricular plane motion relate within the same subject. CardiacNexus reports quantitative coupling features; it does not diagnose pulmonary hypertension, myocardial infarction, diastolic heart failure, dilated cardiomyopathy, or heart failure from a single row.
Anatomical and physiological definition
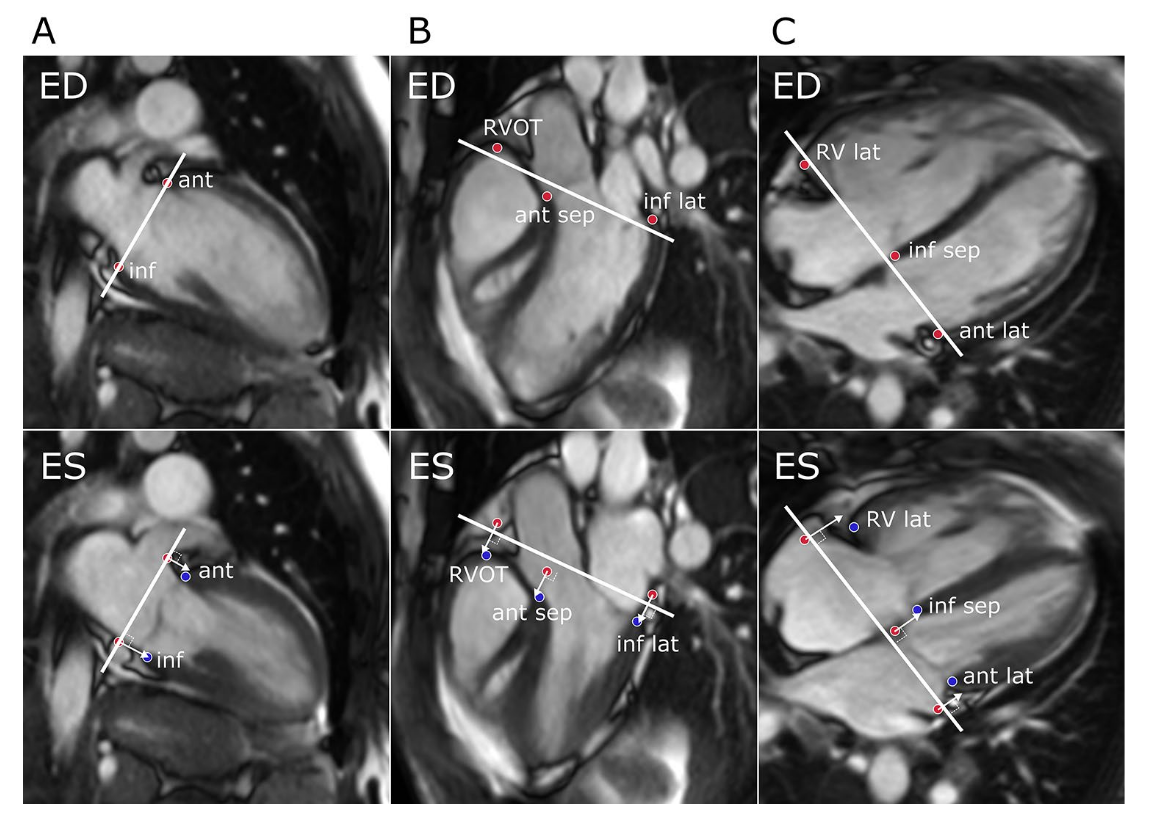
Atrioventricular plane displacement (AVPD) measures systolic descent of the atrioventricular plane. Published CMR protocols often use multi-view LV and RV annular landmarks, whereas the current CardiacNexus row is a simplified 4-chamber implementation [1] [3].
Isovolumetric pulmonary vein transit (IPVT) is the LV stroke-volume component not matched by LA total stroke volume in the same cycle. The IPVT ratio divides this difference by LA total stroke volume, so it is sensitive to both ventricular and atrial measurement quality [6].
Atrial contribution to LV filling estimates the LV filling increment between the ECG-derived LA pre-atrial-contraction frame and LV end diastole, normalized either to LV stroke volume or LV end-diastolic volume [4].
Source acquisition and UKB fields
The current route combines UK Biobank short-axis cine field 20209, long-axis cine field 20208, and ECG-derived atrial timing when available. It requires per-subject images and segmentations, aggregated ventricular and atrial feature CSVs, plus timeseries/ventricle.npz and timeseries/atrium.npz.
What exactly CardiacNexus measures
Atrioventricular plane displacement
eval_ventricular_atrial_feature.py calls evaluate_AVPD on the 4-chamber segmentation at the LV ED and ES frames from the ventricular time series. It writes a single AV: AVPD [cm] row and stores visualization/combined/AV_plane.png when visualization succeeds.
Isovolumetric pulmonary vein transit
The same script computes IPVT as LV: SV [mL] - LA: Total SV (bip) [mL]. If IPVT is negative, the IPVT rows are skipped for that subject. The ratio is IPVT / LA total stroke volume.
Atrial contribution to LV filling
When LA: T_pre_a is available in timeseries/atrium.npz, the script samples LV: Volume [mL] at that frame and compares it with LVEDV and LVESV. If the pre-atrial-contraction LV volume is greater than LVEDV, the atrial-contribution rows are skipped.
Regional contribution boundary
Regional longitudinal, septal, and lateral stroke-volume contributions are important in the CMR literature [2], but they are not emitted by the current CardiacNexus combined-feature CSV. They are therefore documented as a planned/literature boundary, not as current output rows.
Output columns and units
| Display family | Exact output column | Unit | Status | Schema note |
|---|---|---|---|---|
| AV plane displacement | AV: AVPD [cm] | cm | current | simplified 4-chamber implementation |
| IPVT | AV: IPVT [mL] | mL | conditional current | skipped when IPVT is negative |
| IPVT | AV: IPVT Ratio | ratio | conditional current | IPVT divided by LA total stroke volume |
| Atrial contribution | AV: % AC to LVSV [%] | % | conditional current | requires LA: T_pre_a and valid LV volume curve |
| Atrial contribution | AV: % AC to LVEDV [%] | % | conditional current | requires LA: T_pre_a and valid LV volume curve |
Output reconciliation
| Evidence layer | Result |
|---|---|
| Implementation source | 5 current non-valvular combined rows checked against eval_ventricular_atrial_feature.py |
| Output inventory | docs/data/output_column_inventory.yml records ventricular_atrial_feature rows, including the valve rows documented on the valvular page |
| Phenotype dictionary | docs/data/phenotype_dictionary.yml links the 5 cross-chamber rows to this page |
| Page output table | all current cross-chamber rows are listed above |
Required upstream inputs
la_4ch.nii.gzandseg4_la_4ch.nii.gz;timeseries/ventricle.npzwith LV ED/ES frames and LV volume curve;timeseries/atrium.npzwithLA: T_pre_awhen atrial-contribution rows are expected;- aggregated
ventricular_volume.csv; - aggregated
atrial_volume.csv; - consistent subject
eidmembership in both aggregate tables.
Reference ranges with cohort and method context
| Feature | Source | Cohort | Reference value | Status | Note |
|---|---|---|---|---|---|
| AVPD and regional contribution | Ostenfeld et al. [1] | pulmonary hypertension and controls | source-specific values | Verified context source | Multi-point protocol; current row is simplified |
| AVPD prognosis | Lindholm et al. [2] | PAH cohort and controls | source-specific cutoffs | Verified context source | Outcome context, not a CardiacNexus classifier |
| LV pumping contribution | Carlsson et al. [3] | healthy adults, athletes, DCM | method-specific values | Verified context source | Describes AVPD contribution to LV pumping |
| Atrial transport | Rahimtoola et al. [4] | myocardial infarction context | source-specific values | Verified context source | Historical atrial transport-function context |
| Automated CMR workflow | Ruijsink et al. [5] | UKB-scale CMR automation | quality-control context | Verified context source | Supports automation/QC caveat, not direct thresholds |
| IPVT | Aquaro et al. [6] | diastolic dysfunction CMR cohort | source-specific values | Verified context source | Method-compatible context; table-row extraction deferred |
Source-located registry status: reference_range_sources.yml maps AVPD/regional contribution context to Ostenfeld 2016 and Lindholm 2022, LV pumping contribution to Carlsson 2007/2012 context, and IPVT to Aquaro 2019. Because the current CardiacNexus AVPD row is simplified and IPVT depends on paired atrial/ventricular volume curves, these rows remain source-located context rather than diagnostic thresholds.
Disease interpretation
AVPD and regional stroke-volume contribution have been studied in pulmonary arterial hypertension, dilated cardiomyopathy, and heart-failure prognosis [2] [3]. Atrial transport and IPVT relate to myocardial infarction and diastolic filling physiology [4] [6]. The disease badges on this page are interpretation aids only, not validated phenotype-to-ICD classifiers.
QC caveats and maturity boundary
Cross-chamber rows inherit missingness and QC failures from multiple source measurements. IPVT depends on coherent LV stroke volume and LA total stroke volume. Atrial contribution depends on ECG-derived pre-atrial-contraction timing and the LV volume curve. AVPD depends on 4-chamber segmentation quality and ED/ES frame consistency.
The current AVPD output is intentionally labeled as simplified because it does not reproduce the full multi-view LV/RV annular protocol used in several literature sources. Regional longitudinal, septal, and lateral contribution rows should not be shown as current CardiacNexus outputs until the pipeline emits them.
Implementation provenance
| Feature family | Formula or computational route | Exact output columns | Source code file and function | Upstream dependencies | Conditional behavior | QC artifacts | Schema debt |
|---|---|---|---|---|---|---|---|
| AVPD | evaluate_AVPD(seg4_la_4ch, nim_la_4ch, T_ED, T_ES) | AV: AVPD [cm] | eval_ventricular_atrial_feature.py; evaluate_AVPD | 4-chamber cine, 4-chamber segmentation, LV ED/ES frame indices | skipped if helper raises ValueError | visualization/combined/AV_plane.png | simplified 4-chamber AVPD, not full multi-view AVPD |
| IPVT | LV: SV [mL] - LA: Total SV (bip) [mL]; ratio to LA total stroke volume | AV: IPVT [mL], AV: IPVT Ratio | eval_ventricular_atrial_feature.py | ventricular and atrial aggregate CSVs | skipped if IPVT is negative | no dedicated new figure | mixes ventricular and atrial upstream measurement assumptions |
| Atrial contribution | (LVEDV - LV_pre_a) / LVSV and (LVEDV - LV_pre_a) / LVEDV | AV: % AC to LVSV [%], AV: % AC to LVEDV [%] | eval_ventricular_atrial_feature.py | LA: T_pre_a, LV volume time series, LVEDV, LVESV | skipped if timing is missing or pre-A volume exceeds LVEDV | no dedicated new figure | ECG timing availability controls row presence |
| Regional contribution boundary | not emitted by current pipeline | no current output column | not applicable | multi-view long-axis/short-axis regional contribution workflow would be required | literature context only | none | do not add regional rows unless pipeline emits them |
Source audit
- Current AVPD, IPVT, IPVT ratio, and atrial-contribution labels were checked against
eval_ventricular_atrial_feature.py. - Valve diameter rows in the same aggregate remain documented on the valvular page and are not duplicated in this page's feature summary.
docs/data/reference_sources.ymlis present and used as the curated reference-source registry for this page.- Textbook context boundary: implementation, AVPD, atrial transport, automated CMR, and IPVT sources are sufficient for draft rollout; Braunwald/Hurst background was not needed for the phenotype-specific output contract.
- One AVPD measurement panel is displayed from a page-local public path and registered in
docs/data/figure_provenance.yml; permission and exact source-panel review remain pending for draft use.
Related pages
References
- Ostenfeld E, Stephensen SS, Steding-Ehrenborg K, Heiberg E, Arheden H, Radegran G, Holm J, Carlsson M. Regional contribution to ventricular stroke volume is affected on the left side, but not on the right in patients with pulmonary hypertension. The International Journal of Cardiovascular Imaging. 2016;32(8):1243-1253. doi:10.1007/s10554-016-0898-9.
- Lindholm A, Kjellstrom B, Seemann F, Carlsson M, Hesselstrand R, Radegran G, Arheden H, Ostenfeld E. Atrioventricular plane displacement and regional function to predict outcome in pulmonary arterial hypertension. The International Journal of Cardiovascular Imaging. 2022;38(10):2235-2248. doi:10.1007/s10554-022-02616-w.
- Carlsson M, Ugander M, Mosen H, Buhre T, Arheden H. Atrioventricular plane displacement is the major contributor to left ventricular pumping in healthy adults, athletes, and patients with dilated cardiomyopathy. American Journal of Physiology-Heart and Circulatory Physiology. 2007;292(3):H1452-H1459.
- Rahimtoola SH, Ehsani A, Sinno MZ, Loeb HS, Rosen KM, Gunnar RM. Left atrial transport function in myocardial infarction. The American Journal of Medicine. 1975;59(5):686-694.
- Ruijsink B, Puyol-Anton E, Oksuz I, Sinclair M, Bai W, Schnabel JA, Razavi R, King AP. Fully automated, quality-controlled cardiac analysis from CMR: validation and large-scale application to characterize cardiac function. JACC: Cardiovascular Imaging. 2020;13(3):684-695. doi:10.1016/j.jcmg.2019.05.030.
- Aquaro GD, Pizzino F, Terrizzi A, Carerj S, Khandheria BK, Di Bella G. Diastolic dysfunction evaluated by cardiac magnetic resonance: the value of the combined assessment of atrial and ventricular function. European Radiology. 2019;29(3):1555-1564.